I was sent a link to this video and decided to look at the countries mentioned to see what I could find in the data. I normally wouldn’t link to a video but it makes a strong point. It was very revealing.
Vietnam
Here’s what can be found on the US State Department website at the time of this writing:
* According to the Vietnamese Ministry of Health, Vietnam has had 355 confirmed cases of COVID-19 within its borders since the virus first became known.
- 336 people have recovered and were released from the hospital.
- 19 cases are being isolated for treatment.
It has been 77 days without any cases of community transmission in Vietnam; the most recent 88 confirmed cases are all people who arrived in Vietnam with COVID-19 and (like all arrivals) were sent immediately to centralized quarantine. For further details please see the Vietnamese Ministry of Health website here.
* All people in Vietnam are encouraged to wear face masks and avoid close contact with others in public places if possible. All travelers on domestic and international flights must wear face masks during the flight and while at the airport.
KPMG stated on March 20th “the Vietnamese government is currently implementing multiple measures, including travel restrictions, compulsory medical declaration, medical checks, and quarantine upon arrival, with immediate effect. In addition to this, the government is limiting approval for new foreign workers to travel to and work in Vietnam in an effort to reduce external transmission of COVID-19 to Vietnam.”

India
These are some of the measures taken in India according to the US Embassy:
- Prime Minister Modi announced a public curfew on March 22 from 7:00 am to 9:00 pm. On May 1, the curfew was extended until May 18. For the complete guidelines on restrictions, visit the Ministry of Home Affairs webpage, and consult “Guidelines.”
- Following a high level meeting of Indian ministers on March 16, the government proposed extensive social distancing measures, including closure of all schools, museums, and cultural and social centers;prohibiting gatherings of more than 50 people; and calling on the public to avoid all non-essential travel. The complete list of measures can be found here.
- On March 16, 2020 the Government of India expanded compulsory quarantine for passengers coming from or transiting through UAE, Qatar, Oman, and Kuwait. Fourteen-day mandatory quarantine also applies to passengers from China, Italy, Iran, Republic of Korea, France, Spain, and Germany.
- On March 16, 2020 the Government of India prohibited the entry of passengers from the European Union, the European Free Trade Association (Iceland, Liechtenstein, Norway and Switzerland), Turkey, and the UK. On March 17, the government also prohibited the entry of passengers from Afghanistan, Philippines, and Malaysia.
- In addition to the restrictions put in place by the central government, on March 16, Maharashtra Chief Minister Uddhav Thackeray announced mandatory quarantine for travelers from the United States, Dubai, and Saudi Arabia. Other states have announced disparate restrictions as well, including the prohibition of entry of foreigners.
There is much more to the story in India though. According to the Brookings Institution, “After a 14-hour ‘Janata Curfew’ test run, India went into full lockdown on March 24; at the time, India had just 500 confirmed COVID-19 cases and fewer than 10 deaths. The sudden lockdown had a severe impact on millions of low-income migrant workers and daily-wage earners. With no savings and little guidance or financial help from the government, these workers and their families faced food insecurity and hardships that led many to walk hundreds of miles to reach their villages.” This action clearly had the unintended consequences of spreading the disease across the country, which has turned into massive exponential growth in cases.
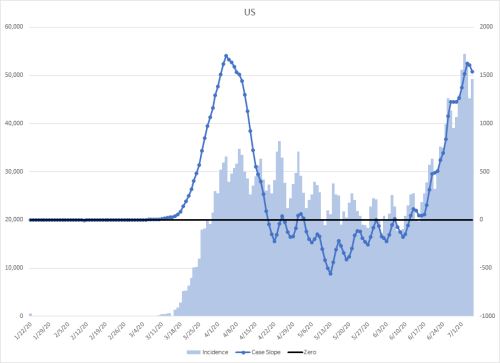
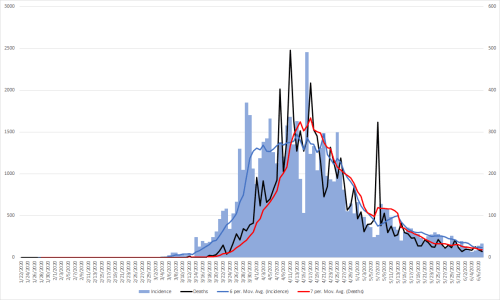
However, there is something to be learned from the data. I had noticed an almost vertical change in the slope of the epidemic curve one day. I’ve changed the scale of the graph to make it stand out and made that particular part of the graph of the derivative slopes red and the three surround areas on either side orange.

What I wanted to know was what had set off this huge leap on May 1st (indicated by the large red dot)? I’ve written earlier how social changes that impact a representative sample of a population take three to show up in the data. Given that information, I could look backward three weeks from May 1st and figure out what happened on whatever day that fell on.
The day three weeks prior to May 1st was April 10th. That didn’t mean anything to me at first and my first idea was to do a search on holidays in India. I was obviously shocked a the result. April 10th was Good Friday. Only 2.3% of the Indian population is Christian. I was puzzled at how such a small percentage of the population could have such a big impact, so I did a simple search using “Good Friday India.”
The first result from that search answered the question.
“Many Christians in India attend special church services or pray on Good Friday. Some people also fast or abstain from meat on this day. Many Christians hold parades or open air plays to portray the last days and hours of Jesus’ life in some areas of India…
…Large prayer meetings and parades may cause local disruption to traffic. This is particularly true in areas with a large Christian population.”
It would be interesting to correlate geographical religious concentrations to increasing cases. Finding this relationship between the data and a social practice is one of the things that makes epidemiology so fascinating to me.

Taiwan

I added the points of emphasis in the quoted section below.
“Lost in the fractious and frankly broken conversation about reopening the economy is a simple truism: containing the virus is the best fiscal stimulus. The U.S. Congressional Budget Office is projecting double-digit contractions in the gross domestic product for 2020 and unemployment rates going up to 16% this year — the highest they have been since the Great Depression. By comparison, Taiwan’s central bank expects growth to slow to about 1.5% for the year, and unemployment has “surged” to 4.1%.
To get the economy moving again, we need a functioning health care system.
A lot can be learned about handling a pandemic — and its aftermath — by looking at the health care systems in other countries. Over the past few years, we have been studying 11 countries to write a book titled, “Which Country has the World’s Best Health Care?” Taiwan was one of the countries we studied, and its successful response to Covid-19 was not a matter of luck. It was the result of careful planning and digital innovation, which the U.S. must learn from.”
Read the whole article though. It’s fascinating.
Of course, we could just stay on the course we are taking in the US, but in my opinion, it’s not a good one to me, especially with our healthcare system on the line.